
Child and Adolescent Psychiatry
Anna Belikova, DO
Resident Physician
Maimonides Medical Center
Brooklyn, New York
Daniel Zhao, MD
Resident Physician
Maimonides Medical Center
New York, New York
Shireen Kazalbasch, n/a
Student Researcher
None
Brooklyn, New York
April Toure, MD
Attending Psychiatrist
Maimonides Medical Center
Brooklyn, New York
Background/Significance: 22q11.2 deletion syndrome, a rare genetic anomaly, presents with diverse symptoms including psychosis, underscoring the necessity for comprehensive psychiatric evaluations and multidisciplinary management approaches (Provenzani et al., 2022). This case report emphasizes the importance of broad differential diagnoses and a holistic view in patient care, with particular consideration of genetic disorders that can present with psychiatric manifestations.
Case: We present a case of a 17-year-old Chinese Mandarin-speaking male with a history of ventricular septal defect, right bundle branch block and hypothyroidism, with no past psychiatric history, who developed early onset psychosis at 15 years old. Between the ages of 15 to 17, the patient underwent several unsuccessful medication trials, including risperidone, chlorpromazine, valproic acid, and sertraline, with only clozapine yielding noticeable improvement in his psychotic symptoms. At the time of presentation, the patient was brought in by his father due to new-onset aggressive behavior. The mental status examination during his initial assessment revealed auditory hallucinations, paranoia, grandiose delusions including a belief of divine identity, bizarre delusions of bodily possession by an unidentified entity, and magical thinking. His condition was further complicated by decreased sleep, nighttime restlessness, and psychomotor agitation, without any depressive or vegetative symptoms. Laboratory tests and medical evaluations did not contribute significant findings. A diagnosis of 22q11.2 deletion syndrome was eventually established following his fourth psychotic episode, underscoring the diagnostic delay caused by an initial oversight of genetic testing.
Provenzani U, Damiani S, Bersano I, Singh S, Moschillo A, Accinni T, Brondino N, Oliver D; Fusar-Poli P: Prevalence and incidence of psychotic disorders in 22q11.2 deletion syndrome: a meta-analysis. International Review of Psychiatry 2022; 34:7-8, 676-688, DOI: 10.1080/09540261.2022.2123273 Zinkstok JR, Boot E, Bassett AS, Hiroi N, Butcher NJ, Vingerhoets C, Vorstman JAS, van Amelsvoort TAMJ. Neurobiological perspective of 22q11.2 deletion syndrome. Lancet Psychiatry 2019 Nov;6(11):951-960. doi:10.1016/S2215-0366(19)30076-8. Epub 2019 Aug 5. PMID: 31395526; PMCID:PMC7008533.
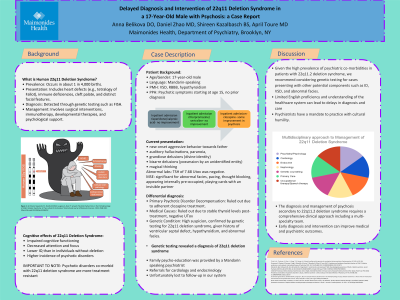
Discussion: The incidence of psychotic disorders in individuals with 22q11.2 deletion syndrome is significant, yet routine testing for genetic disorders in psychiatry remains uncommon (Zinkstok et al., 2022). Genetic testing and early intervention is also limited by patients’ and families’ understanding of both medical and psychiatric illnesses. Approaching psychiatric manifestations of genetic disorders with cultural humility can bridge such misunderstandings (Trinh et al., 2020). This case demonstrates the importance of considering a genetic etiology in early onset psychosis, particularly when accompanied by a history of medical issues.
Conclusion: The diagnosis and management of psychosis secondary to 22q11.2 deletion syndrome demand a comprehensive clinical approach. We recommend a multi-specialty system to patient care and, when possible, early diagnosis and intervention to improve medical and psychiatric outcomes.
References:
Trinh, N. H., Tuchman, S., Chen, J., Chang, T., & Yeung, A.: Cultural humility and the practice of consultation-liaison psychiatry. Psychosomatics, 61 2020; 4:313-320.
Presentation Eligibility: "Not previously published or presented"
Diversity, Equity, and Inclusion: We hope to present a challenging case that revolves around a Mandarin-only speaking patient and his father. Psycho-education was done in Mandarin, however we were faced with addressing certain misconceptions based in the family's ethnic and cultural practices. In our case report, we discuss the need for cultural humility and patient-centered care in the adolescent population. We also encourage the use of translators and figures in the community as a means to engage patients and their families in conversations around mental heal care, expectations of symptom resolution, and the integration of culturally-bounded practices with pharmacological treatment interventions.
