
Cardiology

Yazmin Rodriguez, Bachelor's of Science
Medical Student
Florida Atlantic University
Boca Raton, Florida

Nicholas Smith, Bachelor's of Science
Medical Student
Florida Atlantic University
Boca Raton, Florida

Jake Teich, MD
Psychiatry Resident
FAU College of Medicine
Boca Raton, Florida
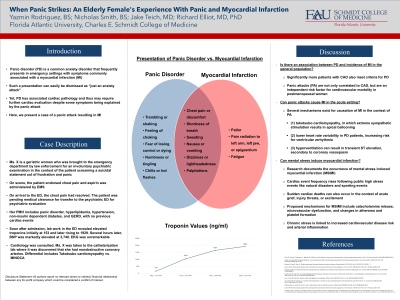
Panic disorder is a common anxiety disorder that frequently presents in emergency settings with symptoms commonly associated with a myocardial infarction. Such a presentation can easily be dismissed as “just an anxiety attack.” Yet panic disorder has associated cardiac pathology and thus may require further cardiac evaluation despite some symptoms being explained by the panic attack. Here, we present a case of a panic attack resulting in myocardial infarction.
Case:
Ms. X is a 67-old woman who suffered from panic disorder superimposed on acute psychosocial stressors. When she was informed that her husband’s Medicare benefits would be discontinued, Ms. X exhibited symptoms of panic attack with reported suicidal ideation prompting a 911 call and subsequent involuntary psychiatric evaluation. Further medical evaluation revealed non-ST elevated myocardial infarction.
Discussion:
Fleet et. al. found that 34% of patients with CAD also met the criteria for PD, significantly higher than the prevalence of PD in the general population (Fleet, 1998). Furthermore, panic attacks (PA) are not only correlated to CAD, but are an independent risk factor for cardiovascular mortality in postmenopausal women (Smoller, 2007).
Aside from the general association between PD and MI, several acute mechanisms exist for direct causation of MI in the context of PA. Well-studied causes include (1) takotsubo cardiomyopathy, in which extreme sympathetic stimulation results in apical ballooning; (2) lower heart rate variability in PD patients, increasing risk for ventricular arrhythmia; and (3) induced hyperventilation can result in transient ST elevation, secondary to coronary vasospasm (Machado, 2016).
There is a wealth of existing research on the presence of mental stress-induced myocardial infarction (MSIMI). There are also multiple reports citing an increase in cardiac event frequency following a public high stress event like natural disasters, sporting events, and national attacks. Multiple mechanisms have been proposed including the effects of increased sympathetic activity and catecholamine release, microvascular dysfunction, and alterations in atheroma and platelet formation (Cannon RO 3rd 2009).
Chronic stress has been shown to play a role in the development of adverse cardiac events. In our case, Ms. X was the sole caregiver to her husband. The associated stress was likely associated with arterial inflammation and increased risk of cardiovascular disease (Tawakol A 2017).
References:
Fleet, RP., Dupuis, G., Marchand, A., Beitman, BD. (1998), et al. Panic disorder in coronary artery disease patients. Journal of psychosomatic research, 44(1), 81–90. https://doi.org/10.1016/s0022-3999(97)00136-0
Smoller JW, Pollack MH, Wassertheil-Smoller S, et al. Panic Attacks and Risk of Incident Cardiovascular Events Among Postmenopausal Women. Arch Gen Psychiatry. 2007;64(10):1153–1160. doi:10.1001/archpsyc.64.10.1153
Machado S, Lattari E, Kahn JP. Possible mechanisms linking panic disorder and cardiac syndromes. Springer eBooks. 2016:185-202. doi:10.1007/978-3-319-12538-1_11
Cannon RO 3rd. Microvascular angina and the continuing dilemma of chest pain with normal coronary angiograms. J Am Coll Cardiol. 2009;54(10):877-885. doi:10.1016/j.jacc.2009.03.080
Tawakol A, Ishai A, Takx RA, et al. Relation between resting amygdalar activity and cardiovascular events: a longitudinal and cohort study. Lancet. 2017;389(10071):834-845. doi:10.1016/S0140-6736(16)31714-7
