
Catatonia
Casey Gilman
Resident Physician
Mayo Clinic-Rochester
Rochester, Minnesota
Sheharyar Sarwar, DO (he/him/his)
Associate Consultant
Mayo Clinic
Austin, Minnesota
Background/Significance
Catatonia is a complex syndrome, characterized by motor, behavioral, attentional, and sometimes autonomic symptoms, that can occur due to medical and psychiatric causes. It often goes unrecognized in medically ill patients (Denysenko, 2018).
Case
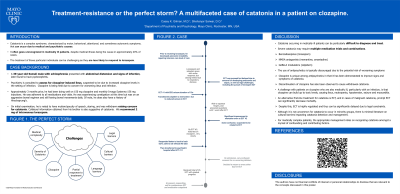
A 39-year-old Somali-speaking male with schizophrenia presented with ileus and pyelonephritis. Psychiatry was consulted for ileus due to increased clozapine levels in the setting of infection. As a result, clozapine was held. Upon evaluation, he had signs and symptoms consistent with catatonia. There was only a partial response to lorazepam challenge and he was transferred to the intensive care unit (ICU) for respiratory distress. In the ICU, lorazepam dosing was limited due to oxygen desaturation secondary to sepsis. Electroconvulsive therapy (ECT) was pursued but delayed due to concern for multifocal infection, as well as cultural and legal challenges, including convincing family to align with treatment team and awaiting emergent ECT permission from the court. As he medically improved, ECT was initiated, although progress was limited by delirium. Reflecting on his hospital course, his treatment resistance was conceptualized as the perfect storm of superinfection, ileus, language, cultural and legal barriers, and partial response to treatment in a catatonic patient on clozapine.
Discussion
Catatonia occurring in medically ill patients is difficult to diagnose and treat. Evidence suggests that delirium and catatonia often co-exist in medical settings and should not be viewed as mutually exclusive. Treatment of these particular individuals is challenging as they are less likely to respond to lorazepam. Additionally, while antipsychotics are typically discouraged due to potential of exacerbating catatonia, clozapine discontinuation is known to trigger catatonia (Denysenko, 2018). A challenge with patients on clozapine who are also medically ill (e.g. infection) is that clozapine can build up to toxic levels, causing ileus, neutropenia, hypotension, seizures and myocarditis (Clark, 2018). An alternative first-line treatment for catatonia is ECT, and in cases of malignant catatonia, prompt ECT can significantly decrease mortality. Despite this, ECT is highly regulated and thus can be significantly delayed due to legal constraints (Shenai, 2016). Although it is not uncommon for catatonia to occur in minority groups, there is minimal literature on cultural barriers impacting catatonia detection and management (Rogers, 2023). For medically complex patients, the appropriate management relies on recognizing catatonia amongst a myriad of confounding and contributing factors.
Conclusions
The following case serves as an example of multiple etiologies that can contribute to or worsen catatonia. It also highlights cultural and legal barriers in the management of catatonia.
References
1) Denysenko, L., et al. (2018). Catatonia in the medically ill: Etiology, diagnosis, and treatment. The Academy of Consultation-Liaison Psychiatry Evidence-Based Medicine Subcommittee Monograph. Annals of clinical psychiatry, 30(2), 140–155.
2) Clark, S. R., et al. (2018). Elevated clozapine levels associated with infection: A systematic review. Schizophrenia research, 192, 50–56.
3) Shenai, N., et al. (2016). Practical and Legal Challenges to Electroconvulsive Therapy in Malignant Catatonia. Harvard review of psychiatry, 24(3), 238–241.
4) Rogers, J. P., et al. (2023). Catatonia: demographic, clinical and laboratory associations. Psychological medicine, 53(6), 2492–2502.
