
Collaborative and Integrated Care
Solomiya Tsymbalyuk, MD (she/her/hers)
Resident physician
University of Maryland Medical Center
Baltimore, Maryland
Valerie Jenkins, MD
Resident Physician
University of Maryland Medical Center
Baltimore, Maryland
.jpg "Samantha Latorre, MD photo")
Samantha Latorre, MD
Associate Program Director, Consultation-Liaison Psychiatry Fellowship
University of Maryland
Baltimore, Maryland

Madeline R. Marks, PhD
Assistant Professor
University of Maryland School of Medicine
Baltimore, Maryland
-Background/Significance: Despite increased national mental health initiatives and expanding access to care, suicide rates continue to rise in the United States (Hedegaard, 2018). Numerous studies have attempted to characterize suicide risk factors, which have largely remained unchanged throughout the past few decades (Franklin, 2017). Data regarding best screening tools to assess suicide risk is limited and heterogenous, underscoring the complexity of accurately assessing, quantifying, and addressing these risk factors (Quinlivan, 2016). Medical teams caring for individuals following a suicide attempt often assume that admission to inpatient psychiatry is the only way to mitigate the individual’s suicide risk. However, psychiatric admission is not always feasible for medically complex patients that may require additional neurologic or physical rehabilitation services for injuries following a suicide attempt.
-
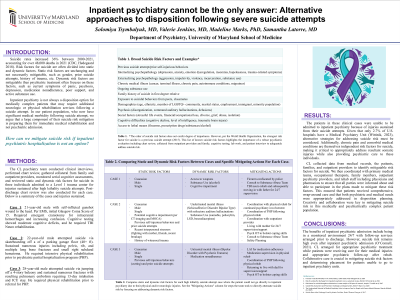
Methods: The consult liaison psychiatry team (CL) conducted clinical interviews, serial cognitive assessments, and reviewed static and dynamic risk factors for suicide in three individuals who were admitted to a Level 1 trauma center for injuries sustained after high lethality suicide attempts. Collaborative efforts were made by CL and primary medical teams to address these risk factors during the medical hospitalization period. Post-discharge chart review was also conducted for each case.
-
Results: The patients in these clinical cases were unable to go to inpatient psychiatry because of their physical or neurological injuries. We discuss each case’s specific suicide risk factors and how CL and primary teams worked to mitigate these risk factors to aid in disposition to physical rehab or neurologic rehab.
-
Discussion: CL collected data from medical records, the patients, families, and outpatient providers to identify mitigatable risk factors for suicide. We then coordinated with primary medical teams, occupational therapists, family members, outpatient psychiatry providers, and rehab staff including physicians and pharmacists to ensure that all parties were informed about and able to participate in the plans made to mitigate these risk factors. This ensured that patients received comprehensive, wrap-around care and that both psychiatric and medical needs were appropriately addressed in disposition planning.
-Conclusion/Implications: The benefits of inpatient psychiatric admission include being in a monitored environment 24/7 with follow-up services arranged prior to discharge. However, suicide risk remains high even after inpatient psychiatric admission (O’Connell, 2021). CL arranged for appropriate psychiatric treatment while patients were receiving care for their medical injuries and appropriate psychiatric follow-up after rehab. Collaborative care is crucial in mitigating suicide risk factors and determining placement for patients unable to go to inpatient psychiatry units.
-
References:
1. Increase in Suicide Mortality in the United States, 1999–2018, Holly Hedegaard et al, 2020
2. Risk factors for suicidal thoughts and behaviors: A meta-analysis of 50 years of research, Franklin et al, 2017
3. Which are the most useful scales for predicting repeat self-harm? A systematic review evaluating risk scales using measures of diagnostic accuracy, Leah Quinlivan et al, 2016
4. Risk of suicide after discharge from inpatient psychiatric care: a systematic review, Patrick H O’Connell et al, 2021
5. Suicide Risk Assessment and Prevention: Challenges and Opportunities, Eileen P. Ryan et al, 2020
