
Diversity, Equity, and Inclusion
 photo")
Caitlin McCarthy, MD (she/her/hers)
Consultation-Liaison Psychiatry Fellow
Medical College of Wisconsin
Milwaukee, Wisconsin
Sara Lindeke, MD
Assistant Professor
Medical College of Wisconsin
Wauwatosa, Wisconsin
Background/Significance: Self-orchiectomy is a rare occurrence primarily documented in the context of psychosis (Garofalo et al., 2018; Kalin, 1979; Lupu et al., 2021). For transgender or non-binary patients with limited access to gender-affirming healthcare, self-orchiectomy may feel like a last resort. We present a case of self-orchiectomy in a non-binary patient without acute psychosis who demonstrated capacity for refusing urological re-attachment of testicles.
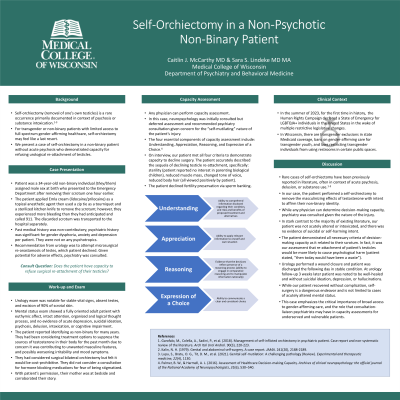
Case: A 34-year-old non-binary individual assigned male sex at birth presented to the Emergency Department after removing their scrotum several hours earlier at home. The patient removed their testicles to eliminate a source of testosterone. The patient used a zip tie as a tourniquet and a kitchen knife to remove the scrotum but experienced excessive bleeding and called 911. Psychiatry was consulted to assess decision-making capacity to refuse testicle re-attachment. The patient was fully oriented with intact attention, organized thought process, and no evidence of psychosis, delusion, or substance use; they denied depression or suicidal ideation and affect was euthymic and mood-congruent. The patient verbalized necessary criterion for decision-making capacity. Urology performed a wound closure and patient was discharged the following day.
Discussion: While rare cases of self-orchiectomy have been reported in literature, the vast majority are in context of psychosis, delusion, or substance use (Garofalo et al., 2018; Kalin, 1979; Lupu et al., 2021). We present a non-binary individual who performed a self-orchiectomy to remove masculinizing effects of testosterone. Urology consulted psychiatry to determine decision-making capacity. The patient was not psychotic, manic, intoxicated, or suicidal. The criteria of decision-making capacity include: understanding of the condition including risks, benefits, and alternatives, ability to appreciate and apply all relevant information, clear reasoning, and expression of a consistent choice (Palmer & Harmell, 2016). Our patient described the sequela of losing their testicles (including sterility, reduced muscle mass, higher voice, and less body hair) and expressed the choice to refuse testicle re-attachment.
Conclusion/Implications: We present a unique case of a non-psychotic, non-binary individual who performed self-orchiectomy to alleviate gender dysphoria. While our patient recovered without issue, self-surgery is a dangerous endeavor. In summer 2023, the Human Rights Campaign declared a state of emergency for LGBTQ+ individuals in the United States in the wake of multiple legislative changes restricting access to inclusive healthcare. This case illustrates that self-orchiectomy is not limited to cases of psychosis or substance use and emphasizes the critical importance of broad access to gender-affirming care.
References:
1. Garofalo, M., Colella, A., Sadini, P., et al. (2018). Management of self-inflicted orchiectomy in psychiatric patient. Case report and non-systematic review of the literature. Arch Ital Urol Androl. 90(3), 220-223.
2. Kalin, N. H. (1979). Genital and abdominal self-surgery. A case report. JAMA. 241(20), 2188-2189.
3. Lupu, S., Bratu, O. G., Tit, D. M., t al. (2021). Genital self-mutilation: A challenging pathology (Review). Experimental and therapeutic medicine, 22(4), 1130.
4. Palmer, B. W., & Harmell, A. L. (2016). Assessment of Healthcare Decision-making Capacity. Archives of clinical neuropsychology: the official journal of the National Academy of Neuropsychologists, 31(6), 530–540.
