
Quality and Safety
 photo")
Margaret Cinibulk, MD (she/her/hers)
CL Psychiatrist
LA General Medical Center, Keck Medicine of USC
Los Angeles, California
Jerry X. Zhao, n/a
Medical Student
University of Southern California
Monrovia, California
Frances Gill, MD
Psychiatry Resident
USC
Los Angeles, California

Talene Keshsihian, M.D.
Chief of Psychiatry at LA General Medical Center
USC
Los Angeles, California
Matthew W. Motley, MD, PhD
Clinical Assistant Professor (Clinician Educator)
Keck School of Medicine of USC
Los Angels, California
Background/Significance: Assistance with management of agitation is a common psychiatric consultation. A 2012 expert consensus, Project BETA, established a validated treatment algorithm for the management of agitation (Roppolo 2020). Inappropriate management, including the excessive use of physical restraints, can result in significant negative health outcomes Further, the etiology of agitation is often not treated pharmacologically. Studies have shown that educational interventions can safely decrease restraint use in nursing facilities (Huizing 2006). Our project aims to improve justification/documentation of physical restraint initiation and selection of appropriate pharmacologic treatment of agitation through educational intervention.
Methods: This study occurred at an academic safety-net hospital with IRB approval. Residency programs and the internist hospitalist group were invited to receive a didactic presentation on managing agitation, including case-based discussions. Participants completed pre- and post-didactic surveys regarding comfort and knowledge of agitation management techniques. A chart review was performed for patients placed into restraints at various 3-month periods (pre-, mid-, and post-didactic intervention). Primary outcome measure of appropriate documentation/justification for initiation of restraint orders and secondary outcome measure of appropriate pharmacologic management of agitation, based on Project BETA guidelines, were compared between the pre-, mid-, and post-didactic intervention periods.
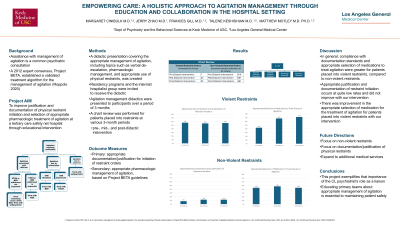
Results: 85 resident and attending physicians participated in didactic presentations. Participants included internal medicine hospitalist attendings and internal medicine/psychiatry/neurology residents. Knowledge scores increased, on average, by 19% after the didactic presentation. On preliminary evaluation, a total of 7, 22, and 32 charts were reviewed during pre-, mid-, and post- didactic intervention periods, respectively. Correct documentation/justification of restraint initiation occurred in 57%, 55%, and 56% of charts reviewed, and percentage of appropriate treatment of agitation with medication occurred in 43%, 68%, and 72% of charts reviewed during the pre-, mid-, and post- didactic intervention periods, respectively.
Discussion: This project exemplifies that importance of the CL psychiatrist’s role as a liaison. While the rate of appropriate documentation/justification for initiation of restraint orders did not change throughout our intervention, there was an increase in appropriate pharmacologic management of agitation. Educating primary teams about appropriate management of agitation is essential to maintaining patient safety.
Conclusion/Implications: While this project supported the role of liaising and educating primary teams to improve management of agitation, areas for improving documentation and selection of pharmacologic agents to manage agitation continue exist. Future directions of this project include expanding the didactic to reach residents in other specialties and to other disciplines, such as nursing.
References:
Roppolo LP, Morris DW, Khan F, et al. Improving the management of acutely agitated patients in the emergency department through implementation of Project BETA (Best Practices in the Evaluation and Treatment of Agitation) [published correction appears in J Am Coll Emerg Physicians Open. 2023 Jun 22;4(3):e13002]. J Am Coll Emerg Physicians Open. 2020;1(5):898-907.
Huizing AR, Hamers JP, Gulpers MJ, Berger MP. Short-term effects of an educational intervention on physical restraint use: a cluster randomized trial. BMC Geriatr. 2006 Oct 26;6:17.
