
Collaborative and Integrated Care
Sherese Ali, MD, FRCPC, ACLP, ABPN (she/her/hers)
Neuropsychiatrist
MacKenzie Health Centre
Toronto, Ontario, Canada
Background/Significance:
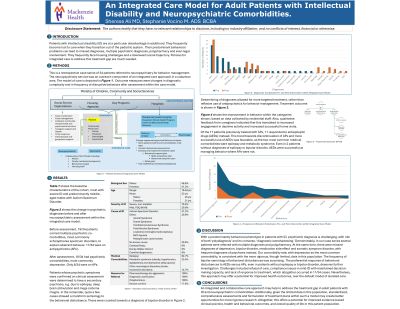
Neuropsychiatric (NP) comorbidity is high in adult patients with intellectual disability (ID) (Cooper, 2015). Their predominant presentation with behavioral problems leads to involvement with the law, multiple psychiatric diagnoses, frequent hospital visits, and treatment with multiple antipsychotics. They frequently face housing challenges and a downward social trajectory. Policies for a comprehensive care model to address this treatment gap are much needed. (Nair, 2022).
Methods:
This is a retrospective case series of 34 patients who were referred for NP consultation, which served as an outreach component of a multidisciplinary care program with a case management approach. This model was inserted into the existing adult mental health service of a community-based program in a suburban area.
Results:
The most common cause of ID was Autism Spectrum Disorder. Most patients had severe ID and were not testable. The remainder had mild ID with FSIQ of 66-69. The most common reason for referral was pharmacotherapy for aggression. Most patients came with a diagnosis of schizophrenia and a history of multiple neuroleptic trials with little benefit.
The model of care allowed for multiple caregiver interviews, comprehensive assessment and regular follow-ups. It was found that most patients’ behaviors were an integral component of the ID syndrome. The next most common diagnosis was psychosis due to a medical condition, such as from multiple brain cavernomata, or epileptic psychosis.
Quantitative data on behavior and seizure frequency showed quite significant improvement, and consequently, an increase in daytime activity engagement. There was an increase in successful home visits based on caregiver and group-home staff reports.
Adherence to care was high with 8/34 patients and/or caregivers declining care.
Discussion:
With a significant treatment gap in this population where medical comorbidity is high, a multidisciplinary, case-management approach provides a good opportunity for access and adherence to care. Some challenges, despite this model, were encountered in patients with mild ID who maintained legal competence and declined treatment. Nevertheless, this integrated care approach has the potential for overall improved health outcomes in this population, versus care that is solely delivered by an individual clinician, with referral based on patient initiative only.
Conclusion/Implications:
A treatment approach towards a more evidence-based integrative model with a case-management component may help to address the treatment gap in adult patients with ID with potential for improved behavior, daytime function, housing status, social trajectory and overall quality of life.
References:
1. Cooper S, McLean G, Guthrie B, McConnachie A, Mercer S, Sullivan F and Morrison J: Multiple physical and mental health comorbidity in adults with intellectual disabilities: population-based cross-sectional analysis. BMC Fam Pract. 2015; 16: 110-121.
2. Nair R, Chen M, Dutt AS, Hagopian L, Singh A, Du M: Significant regional inequalities in the prevalence of intellectual disability and trends from 1990 to 2019: a systematic analysis of GBD 2019. Epidemiology and Psychiatric Sciences, 2022; 31, e91, 1–11.
Presentation Eligibility: Not previously published or presented.
Diversity, Equity, and Inclusion: It is well recognized that adults with Intellectual Disability, who frequently present with aggression and visible deformities, face difficulty with social inclusion. Their inability to communicate suffering in societally acceptable ways contributes to social isolation. They may not enjoy the same access to or quality of care, that an otherwise cognitively healthy adult may be able to negotiate. Additionally, the case series includes a racially diverse population with 14/34 immigrants and non-White Canadians. The author, also a non-White immigrant, aims to advocate for a care model that seeks to improve health care equity for this racially diverse and marginalized population.
