
Psychopharmacology and Toxicology
Rawan Alhau, MD (she/her/hers)
Trainee
Department of Psychiatry and Behavioral Health
Hummelstown, Pennsylvania
Rawan Alhau, MD (she/her/hers)
Trainee
Department of Psychiatry and Behavioral Health
Hummelstown, Pennsylvania

Yassir O. Mahgoub, MD FAPA
Assistant Professor
Penn State College of Medicine
Hummelstown, Pennsylvania
Yassir O. Mahgoub, MD FAPA
Assistant Professor
Penn State College of Medicine
Hummelstown, Pennsylvania
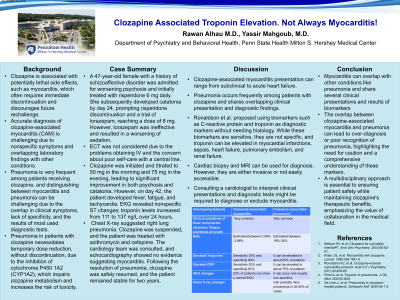
Clozapine is associated with potentially lethal side effects such as myocarditis, which should warrant immediate discontinuation. Accurate diagnosis of myocarditis can be challenging, as symptoms and test values are nonspecific. We present a case of a patient with schizoaffective disorder who developed a transient elevation of troponin during the treatment of clozapine. Further workups, including EKG and echocardiography, didn’t suggest a diagnosis of myocarditis, and clozapine was later resumed safely. Case Summary: A 47-year-old female with a history of schizoaffective disorder was admitted for worsening of psychosis. She was initially started on risperidone 6 mg daily; however, due to developing catatonic symptoms by day 24, risperidone was discontinued. Lorazepam was trialed up to 8 mg daily, with no response. ECT was considered, but due to the patient’s underlying health conditions and poor self-care, intravenous and central lines were regarded as high risk. Clozapine was started on day 35, and the dose was gradually increased to 50 mg in the morning and 75 mg in the evening, with significant improvement in psychosis and catatonia. On day 42, she developed fever, fatigue, and tachycardia. EKG showed non-specific ST changes. Her creatinine kinase level was 12 U/L; troponin increased to 111- >119- >137 ng/L over 24 hours. Chest X-ray showed evidence of right lung pneumonia. Clozapine was initially discontinued due to concerns of myocarditis, and she was treated with azithromycin and cefepime. A cardiology service evaluated the patient, and echocardiography showed no evidence of myocarditis. Hence, clozapine was resumed. The patient remained stable on clozapine for two years without any side effects. Clozapine-associated myocarditis is an uncommon but potentially lethal side effect. The clinical presentation of myocarditis can vary from subclinical or mild symptoms to acute heart failure. Despite cardiac muscle biopsy being the gold standard for diagnosis, it has been disregarded due to procedural risks. Ronaldson et al. proposed using biomarkers, including C reactive protein and troponin, as diagnostic parameters without histology. These biomarkers, although sensitive, are primarily nonspecific. CRP rises in many inflammatory conditions, and increased troponin can be seen in a variety of diseases, such as myocardial infarctions, sepsis, heart failure, pulmonary embolism, and renal failure, with one study showing troponin to be elevated in nearly half of older patients with acute pneumonia similar to the case presented in this report.
Introduction:
Discussion:
Conclusion:
Presentation Eligibility: Not previously published or presented
Diversity, Equity, and Inclusion: It is estimated that around 20-30% of patients with schizophrenia are considered treatment resistance. Clozapine is the most effective medication for treatment-resistant schizophrenia and plays a critical role in promoting equity in mental health care by providing relief to individuals who may not have responded to other treatments. Hence, this case encourages a thorough evaluation of patients before discontinuing Clozapine when there are concerns about adverse effects.
